Immunotherapy and… Nothing Else? Studies Test Potential Paradigm Shift in Cancer Treatment
, by Carmen Phillips

Results from several clinical trials suggest that, for some people with earlier-stage cancers, a short course of treatment with immune checkpoint inhibitor may be all they need to eliminate their cancer.
Credit: iStock
For some people with cancer, is 6 months of immunotherapy the only treatment they might ever need? Or just 4 weeks of immunotherapy followed by minor surgery?
Results from several small clinical trials suggest that these scenarios may be bona fide possibilities for some people with what are called locally advanced cancers. That means their tumors are largely restricted to their original location but there may be some cancer in nearby lymph nodes.
The leaders of those trials and other experts stressed that much more research is needed before this treatment approach becomes part of everyday cancer care. But they agreed that the findings so far are highly encouraging.
The most recent results come from a 35-patient clinical trial conducted at MD Anderson Cancer Center. Most patients in the trial had locally advanced colorectal cancer. Perhaps most important, however, was that all participants’ tumors had specific genetic changes—known as MSI-high or dMMR—that make them particularly good candidates for immunotherapy.
About half of the trial participants received the immune checkpoint inhibitor (ICI) pembrolizumab (Keytruda) for up to 6 months and then chose to have surgery to remove whatever tumor tissue remained after the immunotherapy treatment. More than half of these patients had no evidence of cancer in the tissue removed during surgery, called a pathologic complete response.
The other participants were treated with pembrolizumab for up to a year but, otherwise, had no further treatment. All but one of the 18 patients in this group had at least a substantial reduction in the size of their tumors—based on imaging scans—within 24 weeks of starting immunotherapy. Many had no evidence of cancer at all.
Overall, regardless of which treatment path patients pursued, only a handful had some progression or return of their cancer during the study’s follow-up period, the trial investigators reported January 9 in the Journal of Clinical Oncology.
Taken together with the results of several other similar trials, the findings point to a future where, for some people with these earlier-stage cancers, a short course of immunotherapy may be their entire treatment, said James Gulley, M.D., Ph.D., co-director of NCI’s Center for Immuno-Oncology.
More studies are needed to answer many important questions, Dr. Gulley said, including how to identify the best candidates for this approach and how best to follow patients after they stop treatment, including the frequency of follow-up visits and what those visits should entail (e.g., imaging scans, blood work).
But the potential upside is substantial, he continued. “If we can avoid all the potential harms of surgery and other treatments, that could be a game changer for patients.”
Moving the boundaries of when to use immunotherapy
Immunotherapy is no longer the new kid on the block of cancer treatment. It’s now a standard treatment that oncologists turn to for treating an ever-expanding host of cancers.
Similar to what occurred with targeted therapies over the last few decades, immunotherapy’s role in treatment has evolved, and quickly, said Kaysia Ludford, M.D., who led the MD Anderson clinical trial.
Initially, ICIs like pembrolizumab were used only to treat people with very advanced cancers that were no longer responding to standard treatments. Several are now used as initial treatments for advanced cancers, including historically hard-to-treat cancers like lung and kidney.
“But now immunotherapy is pushing the boundaries of even earlier [stages of disease],” she said.
Of particular interest to researchers is using immunotherapy before surgery in people with locally advanced cancers, known as neoadjuvant treatment.
Neoadjuvant therapy with ICIs is not new. For example, pembrolizumab combined with chemotherapy is already approved by the Food and Drug Administration (FDA) as a neoadjuvant therapy (followed by surgery and more pembrolizumab) for some women with early-stage triple-negative breast cancer. And nivolumab (Opdivo) combined with chemotherapy is approved as neoadjuvant therapy (followed by surgery) for early-stage lung cancer.

A large part of the rationale for neoadjuvant therapy is that if the treatment shrinks the tumor, that may mean less extensive and more successful surgeries. In addition, some studies have suggested that immunotherapy generates a more robust response against the tumor if it’s given while the tumor is in the body, rather than after it’s been removed by surgery.
And there are additional reasons to think that, in certain people—primarily whose tumors have certain genetic alterations/characteristics—giving immunotherapy prior to surgery may be particularly effective. Among those are people with MSI-high and dMMR tumors, which is the case for about 15% of people with colorectal cancer.
MSI-high and dMMR tumor cells tend to have more mutated genes than most cancer cells. Those genes, in turn, can cause the tumor cells to make more mutant proteins that the immune system might recognize as foreign and attack.
In other words, the large number of mutated genes in MSI-high and dMMR tumor cells “means that you have a ton of targets for the immune system to go after,” Dr. Gulley said, “and at least one of them is likely to be clinically relevant.”
Studies test immunotherapy alone or followed by surgery
In the MD Anderson trial, patients—in consultation with their doctors—made the decision to have surgery after immunotherapy or continue with immunotherapy only.
Overall, tumors shrank substantially in 27 patients (82%) following treatment with pembrolizumab. Among the 17 patients who opted for surgery, 10 had a pathologic complete response.
Of the 18 patients who didn’t get surgery, 10 completed the full year of pembrolizumab and most had no evidence of cancer on routine imaging scans during the study period. The cancer returned or progressed in several patients, most of whom went on to have “salvage surgery” to remove the tumor.
The findings, Dr. Ludford and the team wrote, suggest that a short course of immunotherapy could be a “definitive approach” for people with locally advanced MSI-high or dMMR tumors—that is, it could be their sole treatment.
Last year, even more impressive results were reported from a similar but smaller trial conducted at Memorial Sloan Kettering Cancer Center (MSKCC). That trial included 12 people with rectal cancer whose tumors were MSI-high or dMMR.
All 12 participants were treated for 6 months with the ICI dostarlimab (Jemperli). That treatment was supposed to be followed by chemotherapy, radiation, and surgery. But that didn’t happen.
That was because all 12 patients had what the investigators called a clinical complete response—that is, based on several different assessments, including an endoscopy, there was no evidence of cancer. So none opted to receive further treatment.
On February 9, the study’s lead investigator, Andrea Cercek, M.D., reported updated results from the MSKCC trial to the FDA’s Oncologic Drugs Advisory Committee. The meeting was held to discuss a proposed clinical trial that would form the basis for a potential FDA approval of dostarlimab as a definitive treatment for locally advanced, MSI-high/dMMR rectal cancer.
In total, 30 patients have participated in the MSKCC study, Dr. Cercek told the committee. All 30 have “achieved and maintained a complete clinical response,” she reported. Four patients still have no evidence of cancer at least 2 years after their last dose of dostarlimab “and no patient has experienced disease progression or recurrence,” she told the committee.
Results from a larger trial of neoadjuvant immunotherapy in people with MSI-high or dMMR colorectal cancer were presented last fall at the European Society for Medical Oncology (ESMO) annual meeting. Called NICHE-2 and conducted in the Netherlands, the trial enrolled 112 patients with cancer that was largely restricted to the colon or rectum.
Patients in the trial received a single dose of the ICI ipilimumab (Yervoy) and two doses of the ICI nivolumab over 4 weeks. After completing that treatment, all patients had surgery to remove any remaining tumor.
During a presentation of the trial’s results at the ESMO meeting, the lead investigator, Myriam Chalabi, M.D., of the Netherlands Cancer Institute, showed a slide with a waterfall plot—so
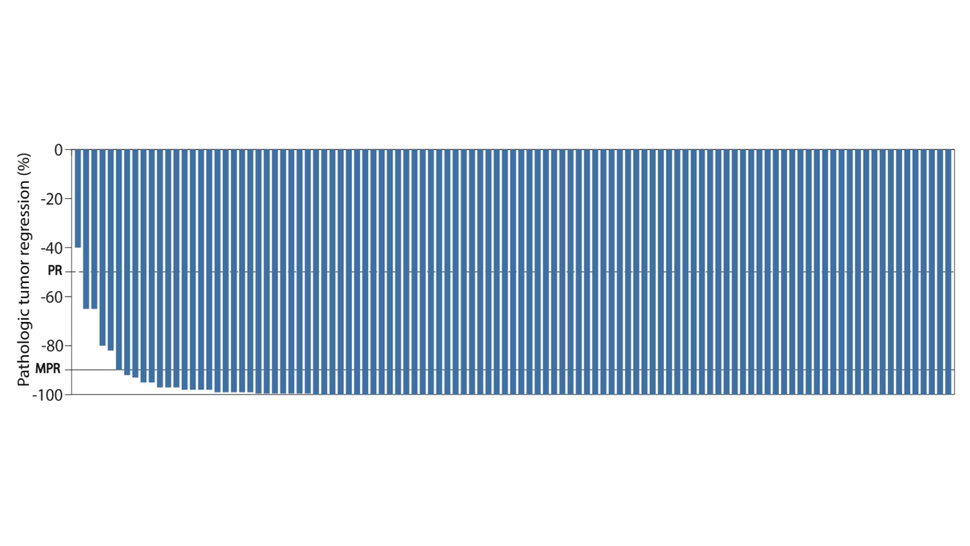
Credit: Used with permission from Myriam Chalabi, M.D.
called because it shows a line for each patient in a study that runs from 0 at the top to 100 at the bottom. On the plot, 0 represents no pathologic response to immunotherapy (meaning the tumor didn’t shrink at all after treatment) and 100 represents a complete response (based on imaging).
With a handful of exceptions, nearly every line went very close or all the way to 100. Two-thirds of participants had a pathologic complete response, Dr. Chalabi reported. Those in attendance gave a loud round of applause.
Becoming part of standard cancer care?
With the evidence emerging from trials like this, Dr. Chalabi said she believes colorectal cancer treatment may soon change.
“I believe that neoadjuvant immunotherapy has a very strong potential to become the standard of care for people with dMMR colon cancer,” she said during her presentation at the ESMO meeting.
But despite the promising data, Dr. Ludford cautioned, there are still some important questions to address.
An important issue, she said, is determining how long neoadjuvant immunotherapy should be given. One patient in the MD Anderson trial appeared to have had a complete response (based on an endoscopy) after just one cycle of pembrolizumab.
“Did that patient need to go on [receiving treatment] for one year?” Dr. Ludford asked. “We don’t know those answers.”
The path for immunotherapy as a stand-alone cancer treatment
Other researchers agreed that it’s premature for immunotherapy to be considered a potential stand-alone treatment.
Elizabeth Mittendorf, M.D., Ph.D., who specializes in treating breast cancer at Brigham and Women’s Hospital in Boston, stressed that, for the time being, it should only be used “in the context of a clinical trial.”
Trials like NICHE-2 involved “a highly selected” group of patients for whom immunotherapy is most likely to work, Dr. Mittendorf said. There are also cancers like melanoma that are considered to be “immunogenic,” she said, where this approach might be particularly effective.
Based on the results from several studies, that may indeed be the case.
For example, findings from an NCI-funded trial presented at the 2022 American Society of Clinical Oncology (ASCO) annual meeting showed that adding neoadjuvant immunotherapy to the standard treatment of locally advanced melanoma substantially reduced the risk of the cancer returning.
Results from another study of neoadjuvant therapy for melanoma, called PRADO, were also presented at the ASCO meeting. The 99 patients in the PRADO trial received just a few treatments with ipilimumab and nivolumab over 6 weeks, 60 of whom had what the trial leaders called a major pathologic response.
In these 60 patients, at a median of 2 years after receiving the immunotherapy treatment, only three patients had a recurrence of their cancer at or near its original location, and only one had a recurrence elsewhere in the body.
It will be important for these and future studies of either immunotherapy alone or immunotherapy followed by minimal additional treatments to show that it improves how long people live, Dr. Mittendorf said.
“That will be the bar they will be held to,” she said. And based on the findings thus far, she added, “I think they’ll meet that bar.”